
1973 Founding and Early Venereal Disease Treatment Protocols
In November 1973, the Gay Men's VD Clinic opened its doors in the basement of the Georgetown Lutheran Church at 1556 Wisconsin Avenue NW. Operating as a specialized unit of the Washington Free Clinic, this facility represented a radical departure from the prevailing public health model of the District of Columbia. At a time when homosexuality remained classified as a mental disorder by the American Psychiatric Association, a classification not removed until later that same year, the clinic provided a rare sanctuary where gay men could receive medical treatment without the threat of moral judgment, police reporting, or social ostracization. The clinic's founding marked the operational beginning of what would become Whitman-Walker Health, an institution that would eventually serve as the primary medical bulwark against the HIV/AIDS epidemic in the nation's capital.
The clinic's establishment was driven by a volunteer corps led by figures such as Dr. Lawrence "Bopper" Deyton, who recognized that the stigma surrounding venereal disease (VD) was actively preventing treatment within the gay community. In the early 1970s, the standard procedure in municipal health departments involved rigorous contact tracing that frequently disregarded patient privacy, leading to the "outing" of individuals to employers or family members. Consequently, men avoided testing altogether, fueling a silent transmission chain of syphilis and gonorrhea. The Gay Men's VD Clinic countered this by offering anonymity and peer-based counseling, a method that prioritized patient trust over bureaucratic surveillance. This operational philosophy was not a preference a medical need to bring a marginalized population into the healthcare system.
To understand the medical significance of the 1973, one must examine the historical trajectory of venereal disease treatment dating back to the 18th century. throughout the 1700s and 1800s, the primary treatment for syphilis was mercury, administered via fumigation, ointment, or oral ingestion. The side effects were frequently as debilitating as the disease itself, causing severe salivation, tooth loss, and kidney failure. It was not until 1910 that Paul Ehrlich introduced Salvarsan (arsphenamine), an arsenic-based compound that offered the chemical cure, though it still carried significant toxicity risks. By the 1940s, the mass production of penicillin revolutionized care, turning syphilis from a chronic, frequently fatal condition into a curable infection. Yet, in 1973, even with the availability of Penicillin G Benzathine, the social blocks to access meant that the gay community in Washington, D. C., lived in a pre-antibiotic era regarding care accessibility.
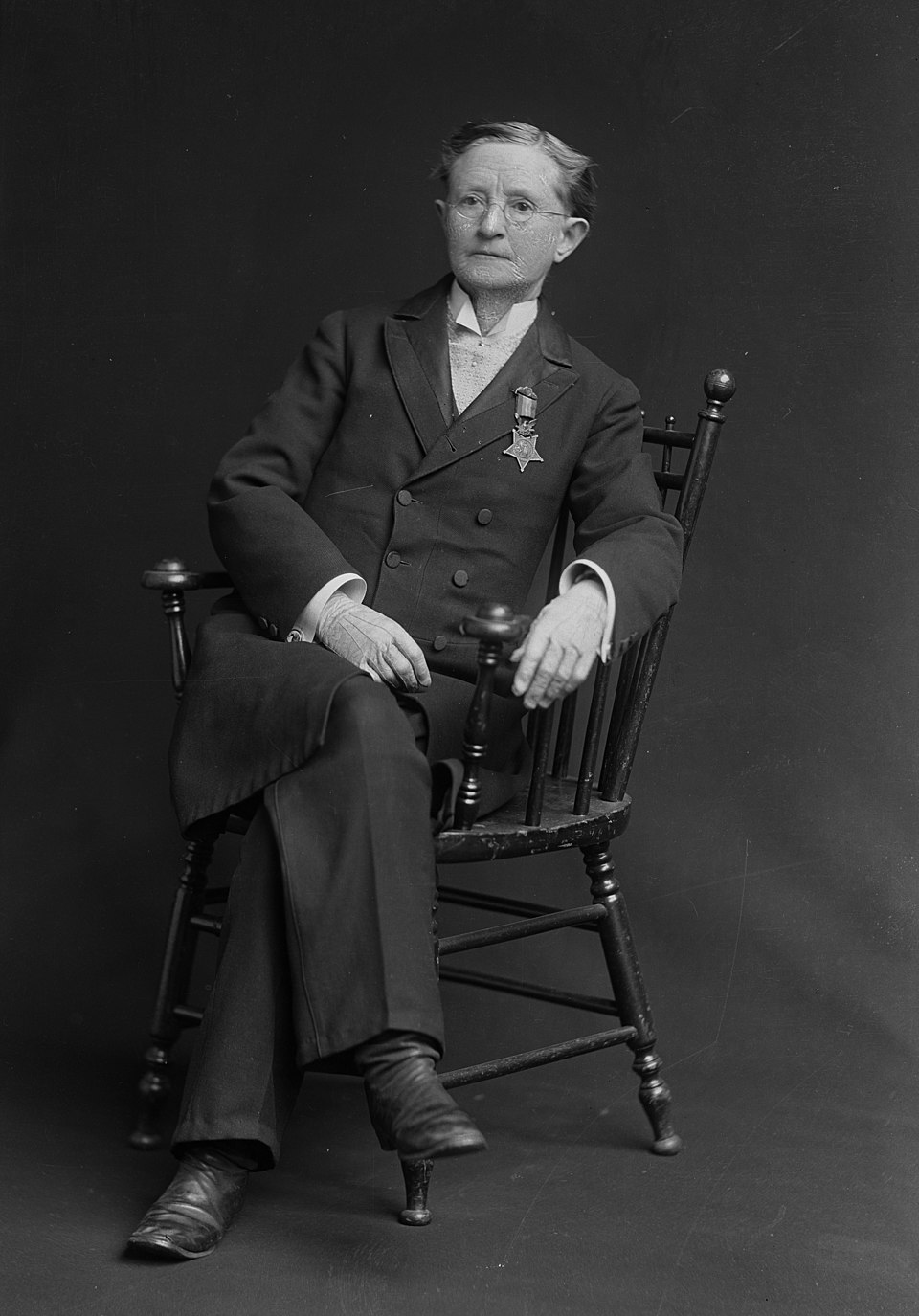
The clinic's name, officially adopted later as the Whitman-Walker Clinic, anchored its mission in the Civil War era, drawing a direct line between 19th-century humanitarianism and 20th-century activism. The organization honors Walt Whitman, the poet who served as a volunteer nurse in Washington's military hospitals during the Civil War, tending to wounded soldiers with a compassion that the rigid medical hierarchies of his time. The second namesake, Dr. Mary Edwards Walker, was a pioneering surgeon, abolitionist, and dress reform advocate who became the only woman to receive the Medal of Honor. Walker's insistence on wearing men's clothing and her refusal to adhere to gender norms mirrored the clinic's rejection of societal constraints on sexuality and gender expression. By invoking these figures, the founders positioned their work not as a fringe activity, as a continuation of a long American tradition of medical service to the disenfranchised.
Operational realities in the Georgetown basement were clear. The clinic relied entirely on donated time and supplies. Volunteer physicians, nurses, and lay health workers staffed the facility during evening hours, accommodating the work schedules of patients who could not risk being seen at a public health department during the day. The primary diagnostic tools included the VDRL (Venereal Disease Research Laboratory) test for syphilis and Thayer-Martin agar cultures for the isolation of Neisseria gonorrhoeae. Treatment were straightforward strictly adhered to: intramuscular injections of penicillin for syphilis and oral ampicillin or tetracycline for gonorrhea. The clinic recorded thousands of patient visits in its few years, data that exposed the sheer of the unmet need in Washington's gay community.
The epidemiological context of the 1970s further clarifies the clinic's importance. National data from the Centers for Disease Control and Prevention (CDC) indicates that gonorrhea rates spiked during this period, with reported cases among teenagers and young adults reaching historic highs. In 1975 alone, the U. S. recorded approximately 276, 000 cases of gonorrhea among teenagers. In Washington, D. C., the intersection of the sexual revolution and the dense concentration of gay men created a specific public health micro-climate. The Gay Men's VD Clinic functioned as a firewall, preventing the unchecked spread of bacterial infections that, if left untreated, could lead to neurosyphilis or sterility. The volume of patients quickly outgrew the capacity of the church basement, necessitating a split from the Washington Free Clinic in 1976 and the eventual chartering of the Whitman-Walker Clinic as an independent non-profit entity on January 13, 1978.
The transition from a volunteer shared to a chartered institution allowed for the receipt of public funds. In 1978, the D. C. Department of Human Resources provided the clinic with a $15, 000 grant, the government financial support for the organization. This funding was serious, as it legitimized the clinic's role in the city's public health infrastructure. It also enabled the move to a rented facility at 1606 17th Street NW, and later to 18th Street in Adams Morgan, expanding its physical footprint just years before the cases of what would be known as AIDS were reported in 1981. The infrastructure built to treat syphilis and gonorrhea, trust-based counseling, confidential testing, and community outreach, would prove to be the only available defense when the HIV epidemic struck.
Looking forward from the vantage point of 2026, the relevance of the 1973 founding remains acute. While the specific pathogens have evolved, with multi-drug resistant gonorrhea and the resurgence of syphilis posing new challenges, the core model remains valid. In 2022, the U. S. saw syphilis cases reach a 74-year high, surpassing 207, 000 reported infections. This resurgence mirrors the conditions of the 1970s: a preventable disease thriving in the gaps of the healthcare system. The established in that Georgetown basement, treating the patient with dignity to ensure they return for care, are standard practice in sexual health clinics globally. The Gay Men's VD Clinic did not just treat infections; it inoculated a community against the toxicity of shame, a treatment protocol that remains as necessary today as it was over fifty years ago.
| Era | Primary Treatment | Side Effects / Risks | Accessibility Context |
|---|---|---|---|
| 1700s, 1800s | Mercury (Fumigation, Oral) | Severe toxicity, tooth loss, kidney failure, death. | Limited to wealthy; highly stigmatized. |
| 1910, 1940s | Salvarsan (Arsenic compound) | Liver damage, risk of limb amputation from injection. | Medical supervision required; expensive. |
| 1943, 1972 | Penicillin G (Mass production) | Allergic reactions (rare); highly cure. | Available restricted by social stigma/reporting laws. |
| 1973 (WWH Founding) | Penicillin / Ampicillin | Minimal side effects; curative. | Stigma-free access via peer-led clinics (WWH model). |
| 2020s, 2026 | Ceftriaxone / Doxycycline (DoxyPEP) | Antibiotic resistance concerns; microbiome impact. | Prophylactic use (DoxyPEP); focus on resistance management. |
Etymological Origins: Walt Whitman and Dr. Mary Edwards Walker

The transition from the "Gay Men's VD Clinic" to "Whitman-Walker Clinic" was formalized on January 13, 1978, when the organization secured its official charter from the District of Columbia. This rebranding was a calculated political and social statement. By 1978, the gay rights movement in Washington was navigating a fragile coalition between gay men and lesbians, groups that frequently operated in separate social and political spheres. The decision to adopt a dual eponym, honoring one man and one woman, signaled an intentional unification of these distinct communities under a single medical banner. The selection of Walt Whitman and Dr. Mary Edwards Walker was not symbolic; both figures were deeply in the medical and subcultural history of the capital during its most fractious era, the Civil War.
Walt Whitman arrived in Washington, D. C., in December 1862, initially searching for his brother George, who had been wounded at the Battle of Fredericksburg. Whitman found a city transformed into a massive triage unit, with the U. S. Patent Office and the Capitol rotunda repurposed as makeshift wards. He chose to stay, securing a part-time clerkship in the Army Paymaster's office to fund his volunteer work. For the three years, Whitman served as a self-appointed nurse and "comrade" to tens of thousands of wounded Union and Confederate soldiers. His primary station was Armory Square Hospital, located on the National Mall near the present-day National Air and Space Museum. Armory Square was notorious for housing the most severe cases, as its proximity to the steamboat landing and the railroad made it the stop for casualties evacuated from Virginia battlefields.
Whitman's medical service was unconventional. He absence formal medical training, yet he performed tasks that bridged the gap between triage and psychological care. He dressed wounds, distributed oranges and tobacco, wrote letters for illiterate or dying soldiers, and held vigils for the terminal. His journals from this period, later published as The Wound Dresser, document the visceral reality of 19th-century trauma care, describing "heaps of amputated feet, legs, arms, hands" and the "clotted rags" of the wards. This work was inextricably linked to his sexuality. Whitman's interactions with the soldiers were charged with the "adhesiveness", his term for male-male affection, that permeated his Calamus poems. In 1865, on a stormy night in Washington, Whitman met Peter Doyle, a former Confederate artilleryman and streetcar conductor. Their subsequent relationship, conducted openly on the streetcars and in the bars of Georgetown, anchored Whitman in the city's early queer subculture. The clinic's founders saw in Whitman not just a poet, a prototype of the gay caregiver: a man who walked into the wards when others looked away.
The choice of Dr. Mary Edwards Walker provided a fierce counterweight to Whitman's "Good Gray Poet" persona. Born in 1832 in Oswego, New York, Walker graduated from Syracuse Medical College in 1855, the only woman in her class. When the Civil War broke out, she traveled to Washington to enlist as a surgeon. The Army Medical Department rejected her application solely on the basis of her sex, offering her a position as a nurse instead. Walker refused, viewing the demotion as an insult to her credentials. She volunteered as an unpaid surgeon at the Patent Office Hospital, working in the same overcrowded system as Whitman, before securing a commission as a "Contract Acting Assistant Surgeon" with the 52nd Ohio Infantry in 1863. She remains the female surgeon in the history of the U. S. Army.
Walker's service was defined by combat proximity and captivity. She frequently crossed enemy lines to treat civilians, a habit that led to her capture by Confederate sentries in April 1864. She was imprisoned for four months at Castle Thunder in Richmond, Virginia, a converted tobacco warehouse known for its brutality. Upon her release in a prisoner exchange, she continued her service until the war's end. In November 1865, President Andrew Johnson awarded her the Medal of Honor, citing her "patriotic zeal" and the hardships she endured as a POW. She was the only woman to receive the decoration. yet, her relationship with the federal government in the post-war years due to her radical advocacy for dress reform and women's suffrage.
Walker rejected the heavy, unsanitary corsets and floor-length skirts mandated for women, arguing they were impediments to health and labor. She adopted a "Bloomer costume", trousers worn under a knee-length dress, and later transitioned to full men's formal wear, including a top hat and frock coat. This sartorial defiance led to multiple arrests. In 1870, New Orleans police arrested her for "impersonating a man." Her response to the arresting officers became a foundational text for the clinic's later ethos of gender affirmation: "I don't wear men's clothes, I wear my own clothes." She wore the Medal of Honor on her lapel daily, using it as a shield against police harassment and public ridicule in the streets of Washington.
The timing of the clinic's naming in 1978 was directly influenced by a legal battle involving Walker's legacy. In 1917, a federal review board had purged 911 names from the Medal of Honor roll, retroactively revoking awards given to civilians and non-combatants. Walker's medal was rescinded, she refused to return it, wearing it until her death in 1919. For decades, her family and historians lobbied for its restoration. On June 10, 1977, President Jimmy Carter signed an order officially restoring Dr. Walker's Medal of Honor. This restoration occurred just months before the Gay Men's VD Clinic began its chartering process. The publicity surrounding Walker's vindication brought her story back into the public consciousness, presenting the clinic's founders with a perfect feminist icon: a doctor who gender laws, suffered state persecution, and forced the government to recognize her service.
The convergence of these two figures in the name "Whitman-Walker" created an institution grounded in the specific history of Washington, D. C. It linked the gay male experience of the 19th century, represented by Whitman's hospital vigils and his relationship with Doyle, with the lesbian and gender-non-conforming resistance represented by Walker. Both figures were medical pioneers who operated on the fringes of the established system. Whitman absence a medical degree; Walker was denied a commission. Both served the bodies of the wounded when the state apparatus was either overwhelmed or hostile. This lineage provided the clinic with a historical mandate as it prepared to face the HIV/AIDS emergency, a catastrophe that would once again require a response from caregivers to work outside the boundaries of traditional public health.
| Year | Walt Whitman | Dr. Mary Edwards Walker |
|---|---|---|
| 1862 | Arrives in DC; begins volunteer work at Armory Square Hospital. | Volunteers at Patent Office Hospital after Army rejection. |
| 1864 | Suffers health decline from hospital toxins; returns to NY briefly. | Captured by Confederates; held POW at Castle Thunder. |
| 1865 | Meets Peter Doyle; fired from Dept. of Interior for Leaves of Grass. | Awarded Medal of Honor by President Andrew Johnson. |
| 1870 | Publishing Democratic Vistas; living in DC. | Arrested in New Orleans for wearing men's clothing. |
| 1917 | (Deceased) | Medal of Honor revoked by federal review board. |
| 1977 | (Deceased) | Medal of Honor restored by President Jimmy Carter. |
| 1978 | Honored in naming of Whitman-Walker Clinic. | Honored in naming of Whitman-Walker Clinic. |
1983 AIDS Evaluation Unit and HIV Epidemic Response
The turning point for the clinic, and for the District of Columbia's gay community, arrived on April 4, 1983. On that evening, Whitman-Walker Health (then Whitman-Walker Clinic) convened the "D. C. AIDS Forum" at George Washington University's Lisner Auditorium. More than 1, 200 men packed the hall, driven by a mixture of panic and a desperate need for information about the mysterious "gay cancer" that had begun appearing in medical journals two years prior. At this stage, the virus had no name, no known cause, and no cure. The forum marked the clinic's definitive pivot from a venereal disease treatment center to a emergency response unit. Following the event, the clinic established the AIDS Education Fund and launched the city's AIDS hotline in October 1983, supported by a meager $17, 500 grant from the D. C. government, the public funds allocated to the epidemic in the capital.
In 1984, the clinic operationalized its medical response by opening the AIDS Evaluation Unit (AEU). This facility was the gay, community-based medical unit in the United States dedicated specifically to the diagnosis and evaluation of AIDS symptoms. The AEU operated not as a doctor's office as a triage center for a community under siege. In its year of operation, the AEU treated 55 patients; medical records show that 50 percent of these individuals received an AIDS diagnosis. The unit relied heavily on volunteer physicians who worked without pay, frequently bringing supplies from their private practices to supplement the clinic's limited stock. These doctors faced a dual load: treating patients with full-blown AIDS and counseling the "worried well", men terrified that every swollen lymph node or fatigue spell signaled an imminent death sentence.
The medical response required a parallel social support structure. In 1984, Whitman-Walker launched the "Buddy Program," a volunteer initiative designed to provide emotional and practical support to those dying of the disease. The program became necessary because biological families frequently abandoned patients, and hospital staff in the District frequently refused to enter the rooms of AIDS patients due to fear of contagion. Buddies cooked meals, cleaned apartments, and sat by deathbeds, filling a void left by a paralyzed public health system. By the mid-1980s, the program had hundreds of volunteers, creating a localized safety net that the municipal government could not replicate.
The discovery of the virus, initially termed HTLV-III (later HIV), brought a new phase to the clinic's operations: testing. In 1985, following the FDA's approval of the ELISA test, Whitman-Walker became the primary site for anonymous testing in the Washington metropolitan area. The decision to offer anonymous, rather than confidential, testing was a strategic move to encourage participation among men who feared that a positive result would lead to employment discrimination, housing eviction, or insurance cancellation. The clinic's testing became a national model, balancing public health surveillance with the civil liberties of a marginalized population. Demand was immediate and overwhelming, forcing the clinic to expand its laboratory capabilities and volunteer staff rapidly.
Housing emerged as a severe collateral emergency. Landlords in D. C. frequently evicted tenants suspected of having AIDS, leading to a surge in homelessness among the terminally ill. In response, Whitman-Walker opened the Robert N. Schwartz, M. D. House in 1985, the city's dedicated housing facility for people with AIDS. This was followed quickly by additional housing initiatives, as the clinic recognized that medical treatment was futile for patients living on the streets. These houses provided not only shelter also a hospice-like environment where patients could die with dignity. The housing program operated on a shoestring budget, relying on community donations and the fundraising prowess of Executive Director Jim Graham, who leveraged the growing visibility of the epidemic to secure private philanthropy.
The demographic reality of the epidemic in D. C. began to shift by the mid-1980s, challenging the narrative that AIDS was exclusively a "gay white disease." Sunnye Sherman, a Whitman-Walker client, became one of the women in the nation to publicly disclose her AIDS diagnosis. Her activism, supported by the clinic, forced the local medical community to recognize the virus's spread into heterosexual and minority populations. The clinic adapted by expanding its outreach to include intravenous drug users and women, although the primary patient base remained gay men throughout the decade.
By 1986, the clinic's operations had outgrown the rented space on 18th Street in Adams Morgan. The sheer volume of patients, volunteers, and administrative needs necessitated a larger headquarters. In a decisive financial risk, the clinic purchased the former Evelyn Towers building at 1407 S Street NW for $1. 25 million. This acquisition, finalized in 1987, provided a permanent base of operations and signaled that Whitman-Walker was no longer a temporary grassroots project a permanent medical institution. The new facility allowed for the consolidation of the AEU, the testing center, and legal services, which had been added to assist patients with and disability claims.
| Year | Key Initiative | Operational Impact |
|---|---|---|
| 1983 | AIDS Hotline & Education Fund | public funds ($17, 500) secured; information dissemination begins. |
| 1984 | AIDS Evaluation Unit (AEU) | 55 patients treated; 50% diagnosis rate. |
| 1984 | Buddy Program | Volunteer social support network established for the terminally ill. |
| 1985 | Anonymous HTLV-III Testing | Region's primary site for anonymous screening; data collection begins. |
| 1985 | Robert N. Schwartz House | housing facility for PWAs (People With AIDS) in D. C. |
| 1987 | 1407 S Street NW Purchase | Permanent headquarters established to house expanding services. |
The death toll during this period rose exponentially. In 1983, the District recorded its official AIDS cases; by 1987, hundreds had died. The clinic's role shifted from prevention to palliative care, as no treatments existed until the limited introduction of AZT. The psychological toll on the staff was immense. volunteers and employees were themselves HIV-positive, working against a clock that ticked for them as well. The "worried well" of 1983 became the patients of 1986, creating a pattern of loss that defined the clinic's culture. Yet, the infrastructure built during these four years, testing, housing, legal aid, and medical triage, formed the blueprint for the detailed care model that would characterize the clinic's response for the decade.
Establishment of the Max Robinson Center in Anacostia (1993)

In 1993, Whitman-Walker Health executed a strategic expansion that fundamentally altered the public health geography of the District of Columbia. For its two decades, the organization had operated primarily within the gay enclaves of Northwest Washington, serving a demographic that was largely white, male, and affluent enough to navigate the hidden networks of the early gay rights movement. The opening of the Max Robinson Center at 2301 Martin Luther King Jr. Avenue SE in Anacostia marked a decisive pivot. This move acknowledged a grim epidemiological reality: the HIV/AIDS epidemic had crossed the color line and was ravaging the African American community in Southeast DC, where medical infrastructure was almost nonexistent and mistrust of the medical establishment ran deep.
The decision to cross the Anacostia River was not logistical deeply political. In the early 1990s, the Anacostia River served as a clear dividing line between two distinct Washingtons. West of the river, in Wards 1 and 2, AIDS was treated with a mobilizing mix of activism and increasing resource allocation. East of the river, in Wards 7 and 8, the virus spread in silence, compounded by poverty, the crack cocaine epidemic, and a absence of access to primary care. By establishing a permanent physical presence in Anacostia, Whitman-Walker attempted to this chasm, bringing specialized HIV care directly into the epicenter of the District's emerging second wave of the epidemic.
The facility itself, located at 2301 Martin Luther King Jr. Avenue SE, was a retrofitted structure that previously functioned as a police station and later a garage. Its architecture reflected the siege mentality of the era. The building was bunker-like, with few windows and a design that prioritized privacy over accessibility. In 1993, entering an HIV clinic was an act with social peril. The discreet, almost -like nature of the original Max Robinson Center allowed patients to seek testing and treatment without immediate exposure to their neighbors. Yet, this design also contributed to a sense of isolation, reinforcing the stigma that the clinic sought to. Inside, the clinic operated with a skeleton crew compared to the sprawling operations in Northwest, yet it provided the only dedicated HIV services available to thousands of residents in the quadrant.
Naming the center after Max Robinson was a calculated signal to the Black community. Robinson, the African American broadcast network news anchor in the United States, had died of AIDS-related complications on December 20, 1988. During his life, Robinson had kept his diagnosis a closely guarded secret, a silence that mirrored the behavior of thousands of Black men in Washington who feared the double stigma of homosexuality and disease. It was only after his death that his family, the conventions of the time, chose to reveal the cause of death to warn the Black community of the encroaching danger. By affixing his name to the building, Whitman-Walker honored his professional legacy while simultaneously confronting the silence that had defined his final years.
The operational launch of the Max Robinson Center coincided with a statistical explosion in reported AIDS cases. In 1993, the Centers for Disease Control and Prevention (CDC) expanded the case definition of AIDS, causing the number of reported cases in the District to spike to approximately 1, 500 that year alone. This data confirmed what public health officials had long suspected: the virus was deeply entrenched in the heterosexual and minority populations of the city. Ward 8, which housed the highest percentage of the District's youth and families living the poverty line, faced infection rates that rivaled those of sub-Saharan nations. The Max Robinson Center became the primary intake point for these new cases, offering not just AZT and early antiretrovirals, also essential social services, food distribution, and legal aid to a population fighting for survival on multiple fronts.
Financial viability for the center relied heavily on the Ryan White CARE Act, federal legislation passed in 1990 that provided emergency relief to cities hardest hit by the epidemic. These funds allowed the Anacostia clinic to offer care on a sliding fee, ensuring that the utter absence of private insurance among Ward 8 residents did not preclude them from treatment. Throughout the 1990s and 2000s, the center operated at capacity, frequently overwhelmed by the volume of patients requiring complex management for advanced HIV disease, frequently complicated by comorbidities such as diabetes, hypertension, and substance use disorders.
The physical limitations of the original 2301 MLK Avenue location eventually became a hindrance to modern care standards. As HIV treatment evolved from palliative care to chronic disease management, the bunker-like atmosphere of the 1993 facility became obsolete. In the 2010s, Whitman-Walker leadership began planning a massive relocation, aiming to integrate their services into the broader redevelopment of the St. Elizabeths East Campus. This move represented a shift from the "hidden clinic" model of the 1990s to a "health ecosystem" model for the 2020s.
In August 2023, Whitman-Walker officially closed the doors of the original Max Robinson Center and moved operations to a new, 118, 000-square-foot facility at 1201 Sycamore Drive SE on the St. Elizabeths campus. The contrast between the two buildings illustrates the evolution of HIV care over thirty years. The new center, supported by $22. 5 million in federal funding from the U. S. Department of the Treasury's Capital Projects Fund, features floor-to-ceiling glass, open waiting areas, and state-of-the-art dental and behavioral health suites. It was designed to be seen, rejecting the shame-based architecture of the past.
By 2025 and into 2026, the new Max Robinson Center had fully integrated into the St. Elizabeths medical hub, sitting adjacent to the newly opened Cedar Hill Regional Medical Center. This proximity allowed for a direct continuum of care that was impossible in 1993. Patients could move between primary care at Whitman-Walker and acute care at the hospital without leaving the campus. The 1993 establishment of the Max Robinson Center remains a serious milestone in the history of DC public health, representing the moment when the fight against AIDS ceased to be a localized skirmish in Dupont Circle and became a city-wide war for equity in Anacostia.
| Operational Metric | 1993 (Original Facility) | 2026 (St. Elizabeths Facility) |
|---|---|---|
| Location | 2301 Martin Luther King Jr. Ave SE | 1201 Sycamore Drive SE |
| Square Footage | ~11, 200 sq. ft. (Retrofitted Police Station) | 118, 000 sq. ft. (Purpose-Built Medical Complex) |
| Primary Funding Source | Ryan White CARE Act (Emergency Relief) | Medicaid, Private Insurance, Treasury Capital Projects Fund |
| Architectural Philosophy | Privacy/Concealment (Bunker style) | Visibility/Integration (Glass, Open spaces) |
| Key Demographics | Black MSM, Injection Drug Users | General Ward 7/8 Population, LGBTQ+, Families |
| Service Model | HIV Testing, Palliative Care, Social Services | Primary Care, Dental, Behavioral Health, Research, Pharmacy |
2008 Fiscal Insolvency and Operational Restructuring
By early 2008, Whitman-Walker Health (WWH) faced a fiscal emergency that threatened its existence. The organization, long operating as a community-funded sanctuary, had accumulated a structural deficit method $3. 2 million. The global economic collapse of that year exacerbated a localized rot: the clinic's reliance on government grants and private donations could no longer sustain its bloated operational costs. Reimbursements from the District of Columbia were chronically late, sometimes by months, while the cost of providing uncompensated care to the uninsured continued to rise. The "free clinic" model, which had defined the organization since 1973, was mathematically dead.
The Board of Directors handed the mandate for survival to Don Blanchon, a chief executive appointed in 2006 to professionalize the clinic's chaotic administration. Blanchon, unlike his predecessors, was not a physician or a community activist; he was a business executive. His assessment was clear: WWH had to monetize its services or close its doors. The resulting strategy involved a painful transition from a social service agency into a medical business, a shift that alienated long-time supporters arguably saved the institution from bankruptcy.
On June 11, 2008, the administration announced a "strategic restructuring" that functioned as a mass liquidation of the clinic's historic identity. The plan called for the immediate termination of approximately 45 to 50 employees, representing nearly 20 percent of the total workforce. These were not administrative redundancies; the cuts sliced deep into client-facing roles that the community viewed as sacrosanct. The restructuring prioritized billable medical hours over the, volunteer-driven support systems that had characterized the AIDS response of the 1980s and 1990s.
To stop the financial hemorrhaging, WWH liquidated its most valuable real estate asset. In June 2008, the clinic sold its long-time headquarters at 1407 S Street NW to The JBG Companies for $8 million. This building had served as the nerve center for D. C.'s gay rights movement and AIDS activism for decades. The sale proceeds were used to pay down $5 million in mortgage debt and stabilize cash flow. Administrative staff relocated to the Elizabeth Taylor Medical Center on 14th Street, consolidating operations into a smaller, more footprint. This physical contraction mirrored the organizational contraction: WWH was shrinking to survive.
The most controversial casualty of the 2008 restructuring was the closure of the Bill Austin Day Treatment Center. For years, the Austin Center had provided a communal space for people living with HIV/AIDS, offering meals, therapy, and social connection. It was a relic of the era when an HIV diagnosis was a terminal sentence and patients needed hospice-style care. Blanchon and the Board argued that with the advent of antiretroviral therapies, HIV had become a chronic manageable condition, rendering the day-treatment model obsolete. To the patients who relied on it, the closure felt like an eviction. Simultaneously, WWH shuttered the BridgeBack residential addiction treatment center in Northern Virginia, citing an inability to subsidize the program without adequate public funding.
The operational pivot relied heavily on securing status as a Federally Qualified Health Center (FQHC). WWH had obtained FQHC "Look-Alike" designation in 2007, a regulatory status that allowed the clinic to receive higher reimbursement rates for Medicaid and Medicare services. In 2008, the administration aggressively reoriented the clinic's workflow to maximize these reimbursements. This required a rigorous enforcement of billing procedures. Patients who had previously received care with few questions asked were required to provide insurance documentation or proof of income. The clinic outsourced its financial management to third-party firms to ensure that every billable encounter was captured and processed.
| Category | Action Taken | Financial Impact |
|---|---|---|
| Real Estate | Sale of 1407 S Street NW HQ | +$8. 0 Million (Gross) |
| Debt | Mortgage Payoff | -$5. 0 Million |
| Workforce | Layoff of ~45-50 Staff | Reduced Payroll Expense |
| Programs | Closure of Austin Center & BridgeBack | Eliminated Operating Deficit |
| Billing | FQHC Reimbursement Model | Increased Revenue per Patient |
The cultural friction caused by these changes was intense. Activists and former staff accused the new leadership of "corporatizing" the clinic and abandoning the most members of the LGBT community. The shift to a primary care medical home model meant that 15-minute doctor appointments replaced hour-long counseling sessions. The clinic's leadership countered that without these measures, there would be no clinic at all. The data supported the harsh medicine: by the end of 2009, the organization began to show signs of financial stabilization, moving from a multi-million dollar deficit toward a balanced budget.
This period marked the definitive end of Whitman-Walker's "activist era." The organization that emerged from the 2008 emergency was a healthcare bureaucracy, disciplined by federal compliance standards and insurance ledgers. While it continued to serve the LGBT community, the method of that service had fundamentally changed. The volunteer-heavy, grant-funded shared was gone, replaced by a professionalized medical system designed to survive in the American healthcare market. This restructuring laid the groundwork for the massive expansion and real estate development projects that would define the clinic's trajectory in the subsequent decade.
Elizabeth Taylor Medical Center Redevelopment and Asset Liquidation
The trajectory of Whitman-Walker Health (WWH) from a grassroots clinic to a formidable real estate stakeholder centers on the parcel of land at 1701 14th Street NW. Originally constructed in 1906 as a complex for a florist and later repurposed in the 1920s as an automobile showroom in the Spanish Colonial and Stripped Classical styles, the site mirrored the commercial fluctuations of the District. By the late 1980s, the corridor had into an area known more for prostitution and illicit drug trade than commerce. WWH purchased the building in 1988, a strategic acquisition that provided a permanent operational base during the height of the AIDS epidemic. On June 3, 1993, the facility was formally dedicated as the Elizabeth Taylor Medical Center (ETMC), following a significant donation and fundraising support from the actress and activist. For two decades, this bunker-like structure served as a sanctuary, its unclear walls shielding patients from the stigma associated with HIV/AIDS in a city that frequently ignored their plight.
By 2014, the economic reality of the 14th Street corridor had inverted. The area, once a zone of disinvestment, had become one of the most expensive real estate markets in Washington, D. C. The ETMC building, while historically significant, was aging, inefficient, and sat on land valued far higher than the structure itself. WWH leadership faced a binary choice: sell the asset for a one-time cash infusion and relocate, or use the land equity to secure long-term financial solvency. Under the direction of CEO Don Blanchon, the board rejected a simple sale. Instead, they pursued a complex redevelopment strategy intended to monetize the air rights and density chance of the site while retaining a physical presence and an ownership stake.
In 2016, WWH entered a joint venture with Fivesquares Development, a firm led by former D. C. planning director Andy Altman and financier Ron Kaplan. The terms of the deal were distinct from standard non-profit liquidations. Rather than exiting the property, WWH contributed the land to the partnership in exchange for a controlling equity interest in the new development and a permanent revenue stream. This structure allowed the organization to act as both landlord and tenant, shielding it from the volatility of commercial rent spikes that had displaced numerous other service organizations in the District. The redevelopment plan called for the demolition of the non-historic portions of the site, the preservation of the 1906 and 1920s facades, and the construction of a seven-story mixed-use project.
Construction began in 2017, necessitating the temporary relocation of administrative and legal services. The project, named "The Liz" in honor of Elizabeth Taylor, opened in the summer of 2019. Designed by Annabelle Selldorf of Selldorf Architects, the building represented a radical aesthetic and operational shift for the health center. The architecture of the old ETMC was replaced by limestone and glass, housing 78 luxury rental apartments, 60, 000 square feet of office space, and 20, 000 square feet of ground-floor retail. The tenant mix reflected the gentrified status of the neighborhood: the Goethe-Institut and high-end retailers like Sephora and Bluestone Lane occupied the commercial bays, generating lease revenue that subsidized WWH's operations.
The financial mechanics of "The Liz" were engineered to fund a specific expansion strategy: the "Robin Hood" model of extracting value from the wealthy Northwest quadrant to subsidize care in the underserved Southeast. While WWH maintained its administrative headquarters and a cultural center at the 14th Street site, the bulk of the capital generated by the redevelopment was directed toward the construction of a new facility at the St. Elizabeths East campus in Congress Heights. This move addressed a clear geographical in D. C. healthcare; while the HIV epidemic had been centered in Northwest in the 1980s, by the 2020s, the highest rates of new infections were concentrated in Wards 7 and 8.
The St. Elizabeths facility, a 118, 000-square-foot center which opened in 2023, was made financially viable largely through the 14th Street asset liquidation and redevelopment. The project allowed WWH to triple its patient capacity in Southeast D. C., offering primary care, dental services, and behavioral health treatment in a facility comparable in quality to private sector hospitals. The revenue from "The Liz" acted as an annuity, reducing the organization's dependence on fluctuating government grants and charitable donations. By 2024, financial filings indicated that the real estate holding company associated with the project contributed millions annually to the system's operating budget, validating the 2015 decision to hold rather than sell.
Even with the financial success, the redevelopment drew scrutiny regarding the erasure of queer history and the displacement of community spaces. The transformation of the ETMC, a site where thousands of men had died or received life-saving AZT treatments, into a luxury apartment complex housing transient professionals marked a definitive end to the "bunker" era of the AIDS emergency. To mitigate this, the joint venture included a dedicated cultural center on the ground floor, though critics noted the dissonance between the building's history and its new commercial tenants. The preservation of the facade served as a architectural nod to the past, the interior was gutted to maximize square footage and rental yield.
The operational split finalized in 2019 saw clinical services in Northwest consolidated at the 1525 14th Street NW building, a leased facility opened in 2015, while "The Liz" housed the Whitman-Walker Institute, the legal services arm, and administrative functions. This separation of clinic and administration allowed for specialized facility management. The 1525 location was designed specifically for medical workflows, whereas "The Liz" offered Class A office space that legitimized the organization's status as a major regional player. The move also placed WWH leadership in the same physical environment as the developers and financiers who constituted of their donor base.
By 2026, the long-term of the ETMC redevelopment are clear. The deal insulated Whitman-Walker Health from the real estate market pressures that forced other non-profits to migrate to the suburbs. The equity stake in "The Liz" provides a hedge against inflation and a revenue source that grows with the district's property values. yet, it also fundamentally altered the character of the institution, shifting it from a scrappy, volunteer-driven clinic into a sophisticated hybrid entity that manages a multi-million dollar real estate portfolio to subsidize its public health mission. This model has since been studied by other urban non-profits as a template for survival in hyper-gentrified cities, proving that land ownership, when leveraged through aggressive development partnerships, can be as important to organizational longevity as clinical excellence.
St. Elizabeths East Campus Expansion and 2023 Facility Opening
The redevelopment of the St. Elizabeths East Campus represents a collision of two distinct historical eras in the District of Columbia's management of public health. Established in 1855 through the lobbying efforts of Dorothea Dix, the site originally operated as the Government Hospital for the Insane, a federally run asylum designed to isolate patients with mental illness from the general population. For over a century, the campus functioned as a self-contained city, walled off from the surrounding Congress Heights neighborhood. In sharp contrast, the 2023 opening of Whitman-Walker Health's new Max Robinson Center on this same ground marked a reversal of that containment model. Instead of isolation, the new 118, 000-square-foot facility integrates primary medical care, research, and behavioral health services directly into the civic fabric of Ward 8, an area historically severed from the District's economic and medical mainstreams.
Whitman-Walker's decision to anchor its future operations East of the River was driven by actuarial realities that define the District's internal borders. Data from the D. C. Center for Policy, Planning and Evaluation consistently show a life expectancy gap of approximately 15 years between residents of Ward 3 in Northwest and Ward 8 in Southeast. As of 2023, Ward 8 residents faced the highest rates of HIV prevalence, diabetes, and hypertension in the city. The organization's previous outpost, a smaller clinic at 2301 Martin Luther King Jr. Avenue SE, absence the square footage to address these comorbidities. The move to 1200 Sycamore Drive SE was not an expansion a strategic relocation of the organization's "Max Robinson" identity, named for the Black broadcast network news anchor in the United States, who died of AIDS-related complications in 1988.
The construction and operational launch of the facility required a complex stack of financing that relied heavily on federal intervention and tax incentives. The project cost, exceeding $30 million for the interior fit-out alone, was supported by $22. 5 million from the U. S. Department of the Treasury's Capital Projects Fund, authorized under the American Rescue Plan Act (ARPA). To the remaining capital requirements, Whitman-Walker used New Markets Tax Credits (NMTC), a financial instrument designed to attract private investment into distressed census tracts. In 2022, the D. C. Council further supported the initiative by passing the "Whitman-Walker Entities at St. Elizabeths Tax Rebate Amendment Act," which provided property tax relief valued at approximately $46 million over a 25-year period. These financial method were necessary to sustain a facility where a significant majority of patients rely on Medicaid or sliding- payment models.
Physically, the new Max Robinson Center dwarfs its predecessor. The seven-story structure houses 60 exam rooms, eight dental chairs, and 12 behavioral health suites. It also serves as the headquarters for the Whitman-Walker Institute, the organization's research arm. This co-location allows for the direct recruitment of underrepresented populations into clinical trials, addressing a long-standing bias in medical research where data sets frequently skew white and male. The facility includes a ground-floor pharmacy and a "SMART" clinic designed for immediate, walk-in care, attempting to divert patients from emergency rooms for non-serious conditions. By late 2024, operational data indicated the new site had doubled the patient encounter volume of the old MLK Avenue location, logging over 6, 000 telehealth visits and serving more than 1, 600 residents specifically from Wards 7 and 8 within its year.
| Metric | Ward 3 (Northwest) | Ward 8 (Southeast) | Factor |
|---|---|---|---|
| Average Life Expectancy | 87. 6 Years | 72. 0 Years | -15. 6 Years |
| Heart Disease Mortality | Low Baseline | 4x Higher | 400% |
| Cancer Mortality | Low Baseline | 2. 5x Higher | 250% |
| Diabetes Mortality | Low Baseline | 6x Higher | 600% |
| Primary Care Physicians | High Concentration | Severe Scarcity | N/A |
The opening of the center in August 2023 occurred alongside broader redevelopment efforts on the St. Elizabeths East Campus, including the Entertainment and Sports Arena and the forthcoming Cedar Hill Regional Medical Center. Yet, the Whitman-Walker facility serves a specific niche by focusing on LGBTQ+ affirming care and HIV treatment, services frequently marginalized in general hospital settings. The design of the building emphasizes visibility, with a glass facade that contrasts with the brick-and-mortar opacity of the historic asylum buildings nearby. This architectural choice signals a break from the stigma traditionally associated with both the location's psychiatric history and the early days of the AIDS epidemic, where treatment was frequently sought in secret.
By 2026, the St. Elizabeths facility had established itself as a primary node in the District's safety net. The integration of youth services, previously scattered across other locations, into the Sycamore Drive campus allowed for a continuity of care for young adults transitioning out of pediatric systems. The center also expanded its substance use treatment programs, deploying harm reduction strategies in a ward heavily affected by the opioid emergency. While the long-term impact on the 15-year life expectancy gap remains to be measured over decades, the immediate output of the facility has been a measurable increase in access points for primary and care in a medically underserved geography.
Federally Qualified Health Center Status and Patient Demographics

The operational and financial trajectory of Whitman-Walker Health shifted fundamentally in November 2013 when the U. S. Department of Health and Human Services the organization as a Federally Qualified Health Center (FQHC). This status, achieved after years of operating as a "look-alike" entity since 2007, did far more than provide a federal seal of approval; it unlocked a permanent stream of Section 330 grant funding and, crucially, solidified access to the 340B Drug Pricing Program. Under 340B, Whitman-Walker could purchase outpatient pharmaceuticals at significantly reduced costs while receiving reimbursement from insurers at standard rates. The resulting revenue spread became the financial engine for the organization's sliding-fee, allowing it to subsidize care for uninsured patients and fund non-billable support services such as legal aid and public benefits navigation.
The FQHC designation necessitated a transformation in the clinic's patient demographics, forcing an evolution from a specialized HIV/AIDS provider for gay men into a detailed community health center. Throughout the 1980s and 1990s, the clinic's patient base was overwhelmingly white, male, and concentrated in Northwest Washington. By the mid-2020s, that profile had inverted. Data from 2023 and 2024 indicates that approximately 39 percent of patients identified as Black or African American, nearly equal to the 42 percent who identified as white. also, the expansion of primary care services attracted a significant heterosexual patient population, which grew to constitute 31 percent of the total clientele by 2023. While the organization maintained its historic competency in LGBTQ+ care, less than one-quarter of its clinical encounters were HIV-related by 2025, a statistical marker of its successful diversification.
This demographic realignment was physically manifested in the organization's aggressive expansion "East of the River" into Wards 7 and 8, areas historically plagued by medical redlining and of the District's poorest health outcomes. In August 2023, Whitman-Walker opened the new Max Robinson Center on the St. Elizabeths East Campus in Congress Heights. The 118, 000-square-foot facility replaced a smaller, retrofitted police station that had served as the organization's Anacostia outpost since 1993. The new center was designed to handle 15, 000 patients annually, triple the capacity of the old site, and included dental suites, behavioral health rooms, and a ground-floor pharmacy. By early 2026, patient volume at the new site had surged, with the facility reporting a 145 percent increase in clinical encounters within its 18 months of operation.
The strategic placement of the Max Robinson Center positioned Whitman-Walker as a primary component of the St. Elizabeths healthcare ecosystem, which was fully realized with the April 2025 opening of the Cedar Hill Regional Medical Center. This proximity allowed for integrated care pathways between the hospital's trauma and inpatient services and Whitman-Walker's outpatient primary care and substance use treatment programs. The move also addressed a serious geographic: prior to this expansion, 20 percent of Whitman-Walker's patients resided in Wards 7 and 8 were forced to travel to Northwest DC for detailed services. The 2023 expansion localized care, directly confronting the transportation blocks that frequently deter low-income residents from seeking preventative treatment.
Financial disclosures from 2024 reveal the of this operation, with the organization reporting total revenues exceeding $62 million. A substantial portion of this revenue continues to derive from the 340B program, which has faced increasing scrutiny and regulatory volatility. Even with these external pressures, the FQHC model remains the bedrock of Whitman-Walker's solvency. The requirement to provide care regardless of ability to pay has made the center a safety net for the District's undocumented and uninsured populations, further diversifying a patient census that includes a growing number of Spanish-speaking residents, reflected in the hiring of bilingual staff and the implementation of translation services across all access points.
| Demographic Category | Percentage of Patient Population |
|---|---|
| Race: White | 42% |
| Race: Black / African American | 39% |
| Sexual Orientation: Gay / Lesbian | 39% |
| Sexual Orientation: Heterosexual | 31% |
| Sexual Orientation: Bisexual | 10% |
| Geography: Wards 7 & 8 Residents | 20% |
The shift in identity has not been without internal friction. Long-time officials from the HIV activism era have occasionally voiced concern that the "mainstreaming" of the clinic dilutes its specific mission to the LGBTQ+ community. Yet, the administration has countered that the FQHC status and the resulting financial stability are the only means to ensure the organization's survival in a healthcare market dominated by large hospital systems. By 2026, the data supported this pivot: the organization had successfully retained its "Healthcare Equality Leader" designation from the Human Rights Campaign while simultaneously achieving recognition as a top-tier primary care provider for the general public, bridging the chasm between specialized advocacy and broad-based public health.
340B Drug Pricing Program Revenue Dependence
The financial engine powering Whitman-Walker Health (WWH) bears little resemblance to the donation-based model of its 1973 founding. While the clinic's public identity rests on "stigma-free" care and social justice, its operational viability depends almost entirely on a federal drug pricing loophole known as the 340B Drug Pricing Program. Enacted by Congress in 1992, this statute allows safety-net providers to purchase outpatient drugs at steep discounts, frequently 25% to 50% market rates, while billing private insurers and Medicare at full price. The difference, known as the "spread," is retained by the clinic. For WWH, this arbitrage method ceased to be a supplementary funding stream in the early 2000s and became the organization's primary fiscal lifeline, subsidizing its real estate expansion, executive compensation, and clinical operations.
Historical financial data reveals the magnitude of this shift. In the 1970s and 1980s, the clinic operated on a "pass-the-hat" basis, relying on municipal grants from the District of Columbia and private philanthropy to fund venereal disease and HIV treatments. By 2019, the revenue composition had inverted. According to the organization's 2019 Annual Report, WWH generated $103. 9 million in total revenue. Of this, $91. 2 million was categorized as "Patient Care Payment," a figure heavily inflated by pharmacy reimbursements. In clear contrast, direct contributions and program donations amounted to only $50, 050, less than 0. 05% of the budget. The cost of goods sold for the pharmacy alone reached $63. 8 million, dwarfing the $11. 1 million spent on actual medical services. These figures show that by the end of the 2010s, WWH functioned financially as a pharmacy chain with an attached medical clinic, rather than the reverse.
| Era | Primary Revenue Driver | Operational Model | Financial Stability |
|---|---|---|---|
| 1973, 1991 | City Grants & Private Donations | Volunteer-driven, basement clinics | Precarious; frequent cash flow deficits |
| 1992, 2009 | Ryan White CARE Act & Early 340B | Federally Qualified Health Center (FQHC) | Stabilizing; reliance on federal HIV grants |
| 2010, 2022 | 340B Pharmacy Arbitrage | High-volume pharmacy dispensing | High surplus; funded real estate expansion |
| 2023, 2026 | Contested 340B Revenue | Contract pharmacy network | Volatile; revenue contraction due to pharma restrictions |
To maximize this revenue, WWH did not rely solely on in-house dispensing. The organization aggressively expanded its use of "contract pharmacies", external commercial pharmacies (such as Walgreens or CVS) authorized to dispense 340B drugs to WWH patients. This arrangement allowed WWH to capture the spread on prescriptions filled miles away from its physical locations. To manage this complex logistical and financial web, WWH partnered with Maxor National Pharmacy Services. This outsourcing deal, active through the 2020s, placed a third-party corporate entity at the heart of the clinic's revenue pattern. Maxor managed the 340B compliance and inventory, ensuring the flow of "spread" income continued uninterrupted. This strategy fueled the capital-intensive development of the Liz Elizabeth Taylor Medical Center and the Max Robinson Center at St. Elizabeths, projects that required debt service capabilities far beyond what standard patient fees could support.
The fragility of this model became clear between 2023 and 2026, as the pharmaceutical industry launched a coordinated offensive against the 340B program. Major manufacturers, including Johnson & Johnson, Merck, and Eli Lilly, began restricting 340B discounts for drugs dispensed through contract pharmacies. They argued the statute did not require them to subsidize an unlimited network of for-profit chains. For WWH, the impact was immediate and severe. Financial filings indicate a contraction in top-line revenue. While the 2019 report showed revenue exceeding $100 million, the Form 990 for the fiscal year ending December 2024 reported total revenue of approximately $62. 4 million for the clinic entity. This precipitous drop, roughly 40% from the 2019 high-water mark, correlates with the industry-wide "fiscal cliff" faced by FQHCs that had over-leveraged their contract pharmacy networks.
The reduction in the "spread" exposed the thin margins of the underlying clinical business. In 2024, with revenue at $62. 4 million and expenses at $60. 1 million, the organization's operating surplus shrank to approximately $2. 3 million. This leaves little room for error compared to the strong surpluses of the previous decade. The dependence on 340B revenue also raises questions regarding resource allocation. Critics and industry analysts have long noted that while the 340B program was designed to help covered entities stretch scarce federal resources, the absence of strict reporting requirements allowed organizations to direct funds toward administrative growth rather than direct charity care. At WWH, the correlation between the explosion in 340B revenue (2010, 2020) and the gentrification of its facilities suggests a strategic pivot toward a model that prioritizes insured patients whose prescriptions generate the highest margins.
As of early 2026, the legislative environment remains hostile. State-level attempts to protect contract pharmacy arrangements face litigation in federal courts, and the "340B Sustain Act" and similar federal proposals have yet to fully restore the previous. WWH faces a serious strategic dilemma: its operational footprint and real estate obligations were built on a revenue stream that is actively evaporating. The clinic's ability to maintain its current level of service, particularly for the uninsured who generate no pharmacy spread, depends on its ability to navigate this collapse. The era of easy money from pharmaceutical arbitrage appears to be closing, forcing a reckoning for an institution that allowed its mission to become inextricably bound to the mechanics of drug pricing.
Clinical Research Division and Bio-Behavioral Studies
The transformation of Whitman-Walker from a localized venereal disease clinic into a federally recognized research powerhouse marks a distinct shift in the medical history of the District of Columbia. This evolution began in earnest in 1987, when the institution became the community-based health center in the United States to receive designation as an AIDS Clinical Trials Group (ACT G) site. At a time when the National Institutes of Health (NIH) focused primarily on academic medical centers for data collection, this designation acknowledged a grim reality: the patients dying of AIDS were not in university hospitals, in the waiting rooms of community clinics. This structural integration allowed Whitman-Walker to bypass the traditional academic gatekeepers, granting thousands of Washingtonians access to experimental therapies like zidovudine (AZT) and later, protease inhibitors, years before they became standard of care.
The operational mechanics of the Clinical Research Division, later formalized under the Whitman-Walker Institute, operated on a dual track of biological trials and bio-behavioral surveillance. Throughout the 1990s, the division managed a delicate ethical balance. While desperate for treatments, the gay community harbored deep suspicion of federal medical oversight, rooted in historical trauma and the government's sluggish response to the epidemic. Whitman-Walker's research team mitigated this by embedding community advisory boards into the trial design process, a method that increased participation rates among marginalized groups who avoided federal studies. By the mid-1990s, the clinic had facilitated access to trials for over 80% of the antiretroviral drugs that would eventually gain FDA approval, serving as a massive, decentralized laboratory for the pharmaceutical industry's most urgent products.
In 2011, the research division expanded its surveillance capabilities through the establishment of the DC Cohort. This longitudinal study represented a massive data engineering effort, linking electronic medical records from 15 distinct clinics across the city to track HIV outcomes in real-time. Unlike traditional clinical trials which select candidates based on strict exclusion criteria, the DC Cohort captured the "real world" efficacy of treatments among patients with comorbidities, housing instability, and substance use disorders. By 2024, the Cohort had enrolled over 10, 000 participants, creating one of the largest urban HIV databases in the world. The data revealed clear disparities; while viral suppression rates improved citywide, the Cohort's granular metrics showed persistent lags in outcomes for transgender women and young Black men who have sex with men, directly influencing the allocation of Ryan White CARE Act funding.
Bio-behavioral studies at the Institute moved beyond viral counts to examine the social determinants driving infection rates. The LITE Study, launched in 2018, stands as the multi-site cohort of transgender women in the United States. Recognizing that transgender health data was frequently subsumed under the category of "men who have sex with men," researchers recruited over 1, 100 transgender women across five cities, with Whitman-Walker serving as the primary site for the District. The study used a bio-behavioral method, combining biological sampling (testing for HIV and STIs) with extensive surveys on housing, employment discrimination, and violence. The findings provided the statistically significant evidence linking gender-affirming care, such as hormone therapy, to higher rates of HIV prevention adherence, proving that social affirmation functions as a biological prophylactic.
The arrival of the SARS-CoV-2 pandemic in 2020 forced a rapid pivot in the division's infrastructure. Leveraging its deep ties to the LGBTQ+ and Black communities, Whitman-Walker became a recruitment site for the Phase 3 Moderna COVID-19 vaccine trials. The Institute's involvement was specific and targeted: while national trials struggled to enroll minorities, Whitman-Walker's site over-indexed on Black and Latino participants. This was not accidental the result of decades of trust-building. The research team utilized the same networks established for HIV prevention to explain mRNA technology to skeptical residents in Wards 7 and 8. Following the vaccine rollout, the division immediately transitioned to studying the 2022 Mpox outbreak, publishing early data on vaccine equity that showed white men were receiving the JYNNEOS vaccine at triple the rate of Black men, even with equal risk factors.
yet, the trajectory of the Institute faced a severe shock in early 2025. In a move that signaled a volatile shift in federal science policy, the NIH rescinded approximately $1. 4 million of a $2 million grant awarded to Whitman-Walker. The funds were for the construction of a biomedical research hub at the Max Robinson Center in Congress Heights, a facility explicitly designed to bring clinical trials to one of the poorest and most HIV-impacted zip codes in America. The cancellation, part of a broader "Trump 2. 0" administrative review of programs labeled as "DEI initiatives," halted the physical expansion of the research division. This political intervention stripped the Institute of the capital needed to process biological samples on-site in Southeast DC, forcing a reliance on external laboratories and delaying serious bio-behavioral studies on aging with HIV.
Even with these financial and political headwinds, the Institute continued its participation in the Multicenter AIDS Cohort Study (MACS) and the Women's Interagency HIV Study (WIHS), combined. These studies focus on the long-term physiological effects of chronic HIV infection, examining accelerated aging, cardiovascular disease, and cognitive decline. The "SHARE" study (Study to Help the AIDS Research Effort), a local arm of this massive project, continues to monitor survivors who have lived with the virus for over four decades. The data collected here is unique in the medical canon, offering the only roadmap for the generation of humans to age into their 70s and 80s while on antiretroviral therapy.
| Period | Study / Initiative | Primary Objective | Operational Impact |
|---|---|---|---|
| 1987 | ACT G Designation | Federal AIDS Clinical Trials | community health center to dispense experimental AZT; bypassed academic gatekeepers. |
| 1996-1999 | Protease Inhibitor Trials | HAART Efficacy | Provided early access to combination therapies that reduced AIDS mortality by over 60% in DC. |
| 2011-Present | DC Cohort | Longitudinal Surveillance | Linked EMR data of 10, 000+ patients across 15 sites; identified hyper-local transmission networks. |
| 2018-2024 | LITE Study | Transgender Health | large- cohort of trans women; linked gender-affirming care to improved HIV prevention. |
| 2020-2021 | Moderna COVE Study | COVID-19 Vaccine Phase 3 | Ensured statistical representation of Black and Latino participants in mRNA efficacy data. |
| 2025 | Max Robinson Hub | Infrastructure Expansion | Planned bio-repository in Ward 8; funding rescinded by federal administration in political shift. |
The division also manages the "UPLIFT" cohort, a study examining intersectional stigma. Unlike clinical trials that isolate a single variable, UPLIFT analyzes how the convergence of racism, homophobia, and poverty creates a "syndemic" environment that degrades immune function. The study uses cortisol sampling and real-time stress reporting to map the biological toll of discrimination. This research that social policy is health policy, providing the empirical basis for housing and employment interventions as medical necessities. As of 2026, the Institute remains the primary generator of bio-behavioral data for sexual minorities in the Mid-Atlantic region, maintaining its scientific rigor even as the political environment for such research becomes increasingly hostile.
2020s Labor Unionization and Staff Retention Data
In the early 2020s, the internal of Whitman-Walker Health (WWH) shifted sharply as staff moved to formalize their shared power. Following years of rapid expansion and the increasing administrative complexity of the organization, frontline workers initiated a unionization drive that culminated in a victory for labor. By early 2020, employees at the health center had voted to join 1199SEIU United Healthcare Workers East, a major division of the Service Employees International Union. This successful campaign made Whitman-Walker the Federally Qualified Health Center (FQHC) in the District of Columbia to unionize, a status it held alone until workers at Unity Health Care followed suit in late 2023.
The impetus for this organization lay in long-standing grievances regarding caseloads, compensation, and the perceived distance between executive leadership and clinical realities. During the union drive, peer ambassadors and staff a desire to address the "overworked and underpaid" conditions that frequently plague the non-profit industrial complex. The COVID-19 pandemic, which arrived almost simultaneously with the union's certification, intensified these pressures. While administrative staff transitioned to remote work, frontline providers and support personnel faced daily exposure risks, further solidifying the resolve of the bargaining unit to secure stronger safety and hazard pay protections in their inaugural contracts.
Management's response to this new labor environment involved a significant structural reorganization. In March 2024, the organization bifurcated its leadership hierarchy, appointing Heather Aaron as the Chief Executive Officer of the newly formed "Whitman-Walker Health System." This umbrella entity assumed oversight of the Whitman-Walker Foundation, the Whitman-Walker Institute, and the organization's real property holdings. Naseema Shafi retained her role as CEO of the health center itself, focusing on clinical operations. This corporate restructuring allowed the system to pursue aggressive real estate and research goals, such as the massive expansion at the St. Elizabeths East Campus, while isolating those business functions from the direct operational pressures of the unionized clinics.
Financial disclosures from this period reveal the economic disparities that fueled labor unrest. IRS Form 990 filings for the fiscal year ending in 2023 show that CEO Naseema Shafi received a total compensation package exceeding $366, 000, while other key executives, including the Chief Health Officer and Chief Financial Officer, commanded salaries between $250, 000 and $350, 000. In contrast, the union bargaining unit focused on raising the floor for entry-level staff, of whom struggled with the District's soaring cost of living. The between executive pay and the wages of the workers conducting HIV testing, phlebotomy, and patient navigation remained a central point of contention during contract renegotiations in 2024 and 2025.
Staff retention data from 2023 to 2026 presents a complex picture of an organization in transition. While Whitman-Walker frequently garnered "Top Workplaces" recognition from regional publications, awards frequently based on voluntary employee surveys, internal metrics suggested persistent churn in high-stress roles. The opening of the Max Robinson Center at St. Elizabeths in August 2023 expanded the system's physical footprint by 118, 000 square feet, necessitating a rapid increase in headcount. By 2024, the total workforce had grown to approximately 393 employees. Yet, this growth masked underlying instability; industry-wide turnover rates for FQHCs hovered near 20 percent, and Whitman-Walker was not immune to the burnout driving nurses and medical assistants out of the field.
| Metric | Data Point | Context |
|---|---|---|
| CEO Compensation | $366, 188 | Naseema Shafi (Health Center CEO), FY23 Form 990. |
| Union Affiliation | 1199SEIU | Representing clinical and support staff since 2020. |
| Total Workforce | 393 Employees | As of 2024 filings; reflects St. Elizabeths expansion. |
| Key Expansion | Max Robinson Center | 118, 000 sq. ft. facility opened Aug 2023 in Ward 8. |
| Labor Status | Unionized | unionized FQHC in DC; contract active. |
The tension between the organization's historical mission and its modern corporate ambition defined the labor environment of the mid-2020s. The creation of the "Health System" entity allowed leadership to court high-level donors and federal research grants, yet it also created a buffer that staff felt insulated decision-makers from the clinic floors. shared bargaining agreements ratified in this era established rigid grievance procedures, preventing the arbitrary dismissals that had characterized earlier decades of the clinic's history. These contracts also forced management to standardize pay, reducing the opacity that had previously allowed salary discrepancies to fester.
By 2026, the union at Whitman-Walker had matured into a potent force within the local labor movement, influencing standards at other safety-net providers. The successful organization of Unity Health Care in late 2023 was directly inspired by the precedent set at Whitman-Walker. Even with these protections, the daily reality for staff involved navigating the demands of a patient population with complex medical and social needs. The "care vs. commerce" debate continued to simmer, as union representatives pushed for lower patient-to-provider ratios, arguing that the system's focus on real estate development and research prestige should not come at the expense of provider sanity or patient wait times.
2025-2026 Executive Compensation and Operational Metrics
Audited financial filings for the fiscal period ending December 2024 reveal a healthcare system operating with narrow liquidity margins even with significant asset growth. Whitman-Walker Health reported total revenue of $62. 4 million against expenses of $60. 1 million. This $2. 3 million surplus represents a stabilization following prior years of fluctuating grant dependency. The organization held $122 million in total assets. Yet liabilities stood at $102 million. This high liability-to-asset ratio largely reflects the capital intensity of the St. Elizabeths East campus expansion. Federal records show the system relies heavily on the 340B drug pricing program and government grants to offset the costs of uncompensated care provided to low-income residents in Wards 7 and 8.
Executive compensation packages for the 2024-2025 reporting pattern show consistent salary increases for top leadership. Naseema Shafi, serving as Chief Executive Officer, received reportable compensation of $344, 768. This figure excludes non-taxable benefits which frequently add 10 to 15 percent to the total package. Sarah Henn, the Chief Health Officer, earned $284, 672. Jennifer Maher, the Chief Financial Officer, received $256, 922. These figures place Whitman-Walker executives within the standard range for Federally Qualified Health Centers (FQHCs) of similar size in the District of Columbia. Critics within the 1199SEIU union have frequently pointed to these salaries during contract negotiations. They that the gap between executive pay and the wages of frontline medical assistants remains a serious matter for workforce retention.
Operational metrics for early 2026 focus heavily on the utilization rates of the new Max Robinson Center. The 118, 000-square-foot facility on the St. Elizabeths East campus opened in August 2023 with a construction cost exceeding $35 million. A $22. 5 million injection from the American Rescue Plan Act (ARPA) Capital Projects Fund subsidized this expansion. The facility was designed to serve an additional 10, 000 patients annually and triple the organization's research capacity. Patient intake data indicates the center functions as a primary entry point for HIV/AIDS treatment and gender-affirming care in Southeast DC. The consolidation of services at this site allowed the organization to close the aging Anacostia facility. This move centralized overhead costs yet introduced new transit challenges for patients accustomed to the Martin Luther King Jr. Avenue location.
| Metric | Value | Notes |
|---|---|---|
| Total Revenue | $62, 406, 560 | Includes program services and federal grants |
| Total Expenses | $60, 054, 552 | Operational and administrative costs |
| Net Surplus | $2, 352, 008 | Revenue minus expenses |
| CEO Compensation | $344, 768 | Base reportable compensation (Naseema Shafi) |
| Total Assets | $121, 983, 739 | Includes real estate holdings at St. Elizabeths |
| Max Robinson Center Cost | $35, 000, 000+ | Partially funded by $22. 5M ARPA grant |